“Despite the fact that the vast majority of health care takes place in the outpatient, or ambulatory care, setting, efforts to improve safety have mostly focused on the inpatient setting.”1
This was the topic of discussion in August when CHPSO and HQI were privileged to share the arena with Anjana Sharma, MD, an assistant professor at the University of California, San Francisco during a webinar on ambulatory patient safety. Dr. Sharma is a primary care physician and researcher in the Department of Family and Community Medicine, where she works passionately to understand the impact of patient engagement in health care and to identify strategies to improve quality and safety within the ambulatory/community setting.
To set the agenda for the mixed-methods analytical probe into ambulatory care safety events, Dr. Sharma kicked off the webinar with three core research questions.
- What types of adverse events are reported in ambulatory safety reporting systems?
- What incidents are associated with significant harm?
- What is the role of patients, families, and caregivers within outpatient safety adverse events?
Of note, the backbone of this study was conducted and supported by a team of clinicians, caregivers, and patients referred to as PARTNRS Study Stake holder Research Advisory Council. The group examined ambulatory events from CHPSO’s database for the period of 2012-18. Event data were dual-coded (random 20%) and the remaining were independently reviewed. A final sample of 2,701 patient safety events was entered into an electronic abstraction form for analysis.
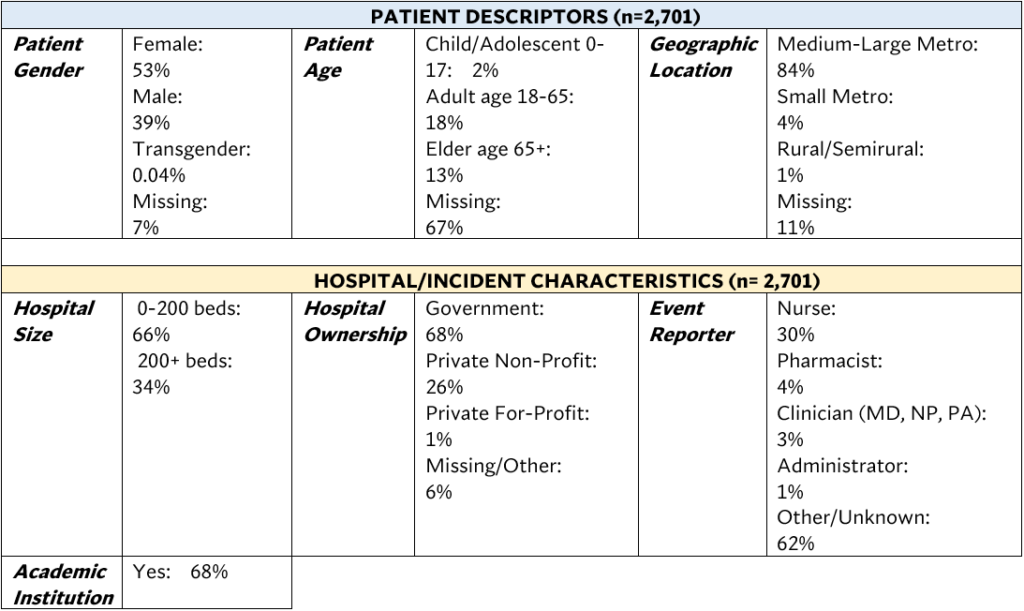
Table 1 shows the patient demographics and hospital/incident characteristics for the event sampled reports. Although the descriptors and characteristics may not appear to be a fair representation of all U.S. patients and hospitals, there are intrinsic limitations with a voluntary safety reporting system. Still, despite these constraints, useful trends and correlations can be culled. Moreover, Dr. Sharma emphasized the need for report submitters to close the gap on missing data by including core variables such as gender, age, and event reporter role, to mitigate bias and false conclusions.
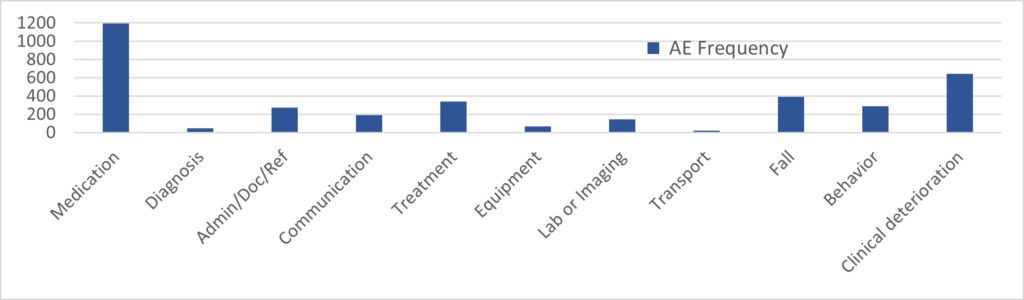
The harm scale results among the sampled data were of normal distribution, i.e., bell-shaped curve, with the top three harm levels classified as moderate harm, mild harm, and no harm, respectively2 The most frequently reported adverse event involved medication errors, followed by clinical deterioration, and falls, which somewhat reflect what we would find in the inpatient setting (Figure 1).
Dr. Sharma noted that among medication class, chemotherapy/immunogenics were associated with the most frequently reported adverse medication events and likely derived from patient encounters within infusions centers; anticoagulants and antibiotics were second and third highest, respectively. However, when it involved high harm events, opioids, hypoglycemics, and anticoagulants, were considered to be the most common high-risk outpatient medications.
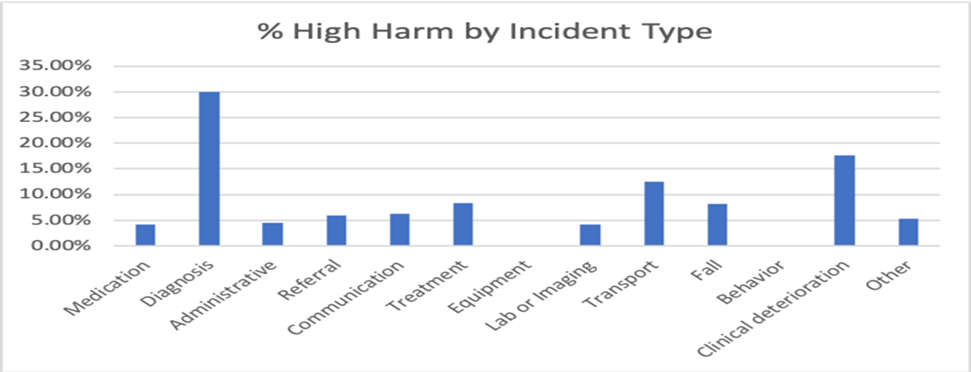
Interestingly, drilldown into the highest harm by incident targeted events associated with the most serious harm (Figure 2). Medication — despite being the most frequent incident — is not necessarily linked to high harm, comparatively speaking. Instead, diagnosis was the incident with the highest harm level at 30%. Likewise, clinical deterioration was the second-highest harm incident and also the second-most frequent adverse event, as shown in Figure 1 above.
Dr. Sharma then presented several examples of incident categories with high harm. One particular event involved a delayed diagnosis:
“Patient had prostatitis, and elevated PSA. Doc future-ordered a repeat PSA 2 months following in 2013. This lab was drawn by lab tech and then cancelled (it was drawn too early). Not reordered, doc not notified. Pt re-presented 818 days later with prostate cancer. Could have been diagnosed early.”
The third and final question is an area that requires further research as it involves complexities surrounding social determinants of health, communication between provider/caregiver/patients, comorbidities, mental health, and other intricate pathways that often lead to adverse events.
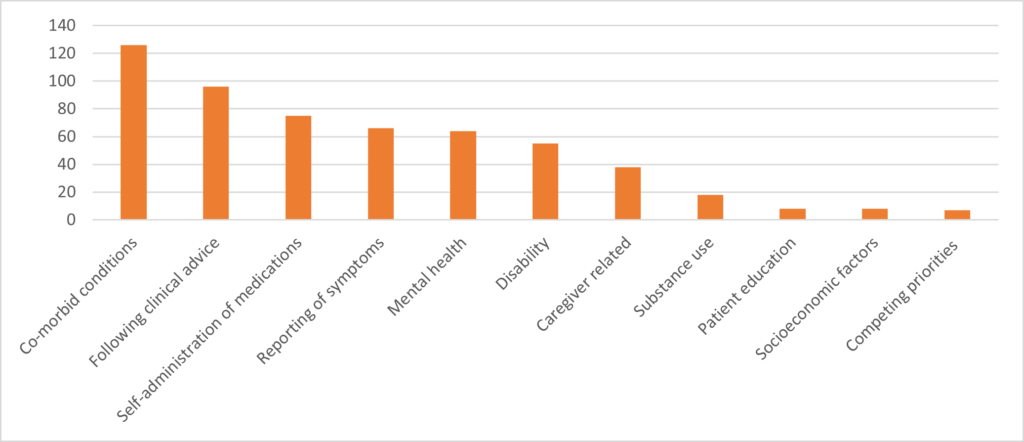
Figure 3 describes and quantifies the frequency of selected themes identified as contributing factors that lead to harm involving both patients and caregivers. Much of the study focused on examining ambulatory harm events from the patient/caregiver’s perspective since adverse event reporting is routinely generated by health care staff and therefore centered from the mindset of the provider. For example, in cases where conflict exists between clinical advice and competing priorities, co-occurrences such as signing out against medical advice or choosing not to go to the emergency room when reporting a symptom are some of the actions/inactions that can lead to adverse events.
Another theme is socioeconomic factors such as the inability to seek care due to lack of transportation, housing issues, or family responsibilities. Other notable challenges that can lead to adverse events include communication failures, such as when pharmacies do not notify patients about medication regimen changes made by their physician or share relevant information such as drug-drug interactions. In situations when diabetic patients are scheduled for an outpatient procedure and instructed not to eat, potential complications such as hypoglycemia can be the result if the patient fails to adjust their insulin dose. Patient education is integral in the area of medication self-administration.
Inarguably, patient and caregiver challenges are multifactorial. With complex conditions/situations such as comorbidities, competing priorities, environmental, psychosocial, and other variables in the ambulatory setting equation, events can morph into unexpected pathways. “The patient and caregiver factors identified in this dataset are both ‘structural’, such as disability, mental health, or socioeconomic factors, as well as ‘behavioral’, such as following clinical recommendations, self-administration of medications and competing priorities.”3
Dr. Sharma concluded her presentation noting that the current ambulatory system is not adequate to monitor patients in primary care or outpatient settings. Medication remains a vulnerable area that requires more pharmacovigilance and oversight. Likewise, it’s imperative that we continue to study and conduct root cause analyses on diagnosis-related events. Lastly, the area of patient and caregiver challenges are correlated with harm and as such, demand that we see these events through their lens. Only then can we begin to move the needle and make a difference in ambulatory patient safety.
The webinar recording and presentation are available online. CHPSO’s 2021 Annual Report is also available.
