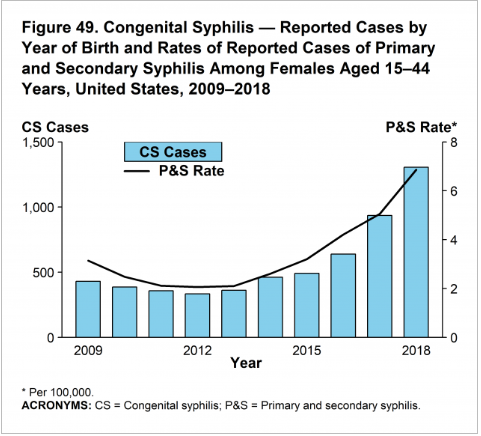
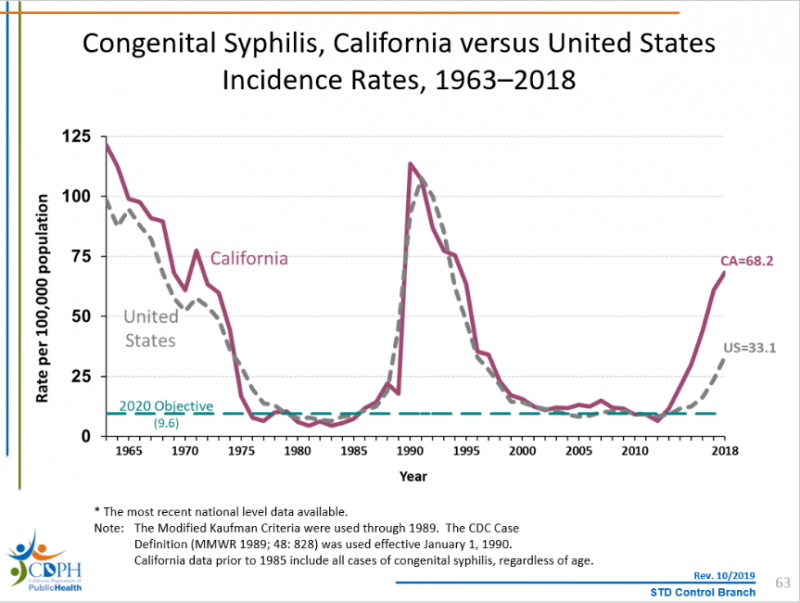
After historic low rates in 2000-2001, California is seeing a resurgence of congenital syphilis. Naturally, congenital syphilis rates closely mirror primary and secondary syphilis rates among females aged 15-44.
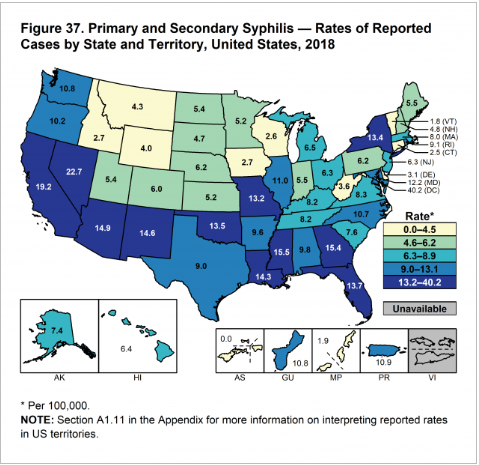
According to Centers for Disease Control and Prevention 2018 data, California had the second highest rate of reported cases (19.2 per 100,000) and the highest number of reported cases (7,607 cases) in the United States.
How does the Hospital Quality Institute (HQI) fit into this picture?
HQI is working toward bringing stakeholders together to help address congenital syphilis. We have identified the geographic areas, population demographics, and member facilities most affected, and we are reaching out to help bridge the information and cooperation gap between member hospitals, health care professionals, public health partners, and their communities. We are seeking information from local health officers (LHOs) and we are compiling and sharing this information with our member hospitals to ensure that these important stakeholders are aware of LHO recommendations. Success in reducing congenital syphilis is not an easy lift, and it requires cooperation across health care facilities, health care providers, and state and local public health teams.
What is congenital syphilis?
Congenital syphilis is an infection transmitted from mother to child during pregnancy and/or delivery caused by the bacterium Treponema pallidum. Congenital syphilis can cause severe illness in babies including premature birth, low birth weight, birth defects, blindness, and hearing loss. It can also lead to stillbirth and infant death…In 2017, most female early syphilis cases and congenital syphilis cases in California were reported from the Central Valley; however, an increasing number of counties throughout California are reporting their first CS case in years. Most women who gave birth to babies with congenital syphilis received prenatal care late in pregnancy or not at all.
What can hospitals and health care facilities do now?
Given that congenital syphilis is passed vertically from mother to baby, current national and state public health directives encourage a focus on identification and treatment of syphilis in the pregnant woman before delivery. While there are numerous barriers to getting some pregnant women into adequate prenatal care, there may be health care interactions— perhaps unrelated to pregnancy— which provide the opportunity for syphilis intervention, such as emergency department (ED) visits. In an environment which is already severely resource limited, it helps to focus on persons most likely to need syphilis testing and treatment. There are several risk factors that seem to be associated with increased likelihood of syphilis and consequently increased likelihood of delivering a baby with congenital syphilis:
- Receiving late or limited prenatal care
- New or multiple partners
- Suspicion that a recent partner may have had concurrent partners
- Partner with male partners
- New STD diagnosis in pregnancy
- Sex partner diagnosed with an STD
- Commercial sex
- Drug use
- Living in an area with high syphilis prevalence among women
SB 1152, which took effect last year, amended Section 1262.5 of the Health and Safety Code to direct hospitals to include screening for infectious disease in their discharge plans specific to homeless patients:
(6) The homeless patient has been offered or referred to screening for infectious disease common to the region, as determined by the local health department.
Some California counties have specific requirements or recommendations from their local health officers (LHOs) regarding testing the homeless population for infectious disease, calling out syphilis (among others). Other counties may have guidance regarding syphilis and other diseases, unrelated to homeless. Please consult your LHO for more information.
County-level guidance:
- Alameda (combined with City of Berkeley)
- Amador
- Butte
- Contra Costa
- Fresno
- Kern County
- Kings County
- Los Angeles County
- Sacramento County
- Sonoma County
