New analysis from HQI examines the changes in adverse outcomes and complications associated with inducing labor for babies that are large for their gestational age, suggesting that early recognition is critical — and later interventions (inducing labor after 39 weeks) may actually worsen outcomes.
When a clinician suspects a baby is larger than average for its gestational age, the common strategy is to induce labor early (often at 38 weeks). This allows the baby to be delivered when it is smaller, preventing shoulder dystocia (a complication wherein a baby’s shoulders get stuck during delivery) and reducing the risk of additional complications, such as fractures or hypoxia for the infant and uterine rupture or postpartum hemorrhage for the mother. However, induction — the use of medications to start labor — also carries specific risks and side effects for both mother and baby.
A landmark 2025 Lancet study — the Big Baby trial — rigorously evaluated this approach and found no meaningful difference in shoulder dystocia rates between induced and non-induced deliveries among randomized cases, including mothers who delivered earlier than planned. It also found that induced delivery led to shorter post-delivery hospital stays and reduced postpartum hemorrhage, but caused a slight increase in second-degree perineal tears.
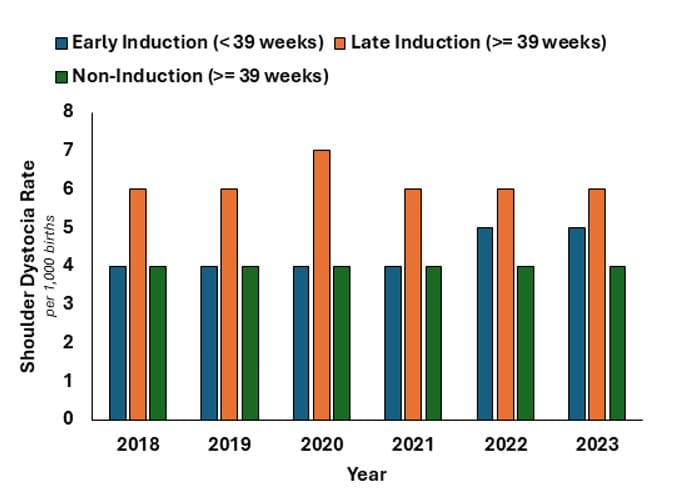
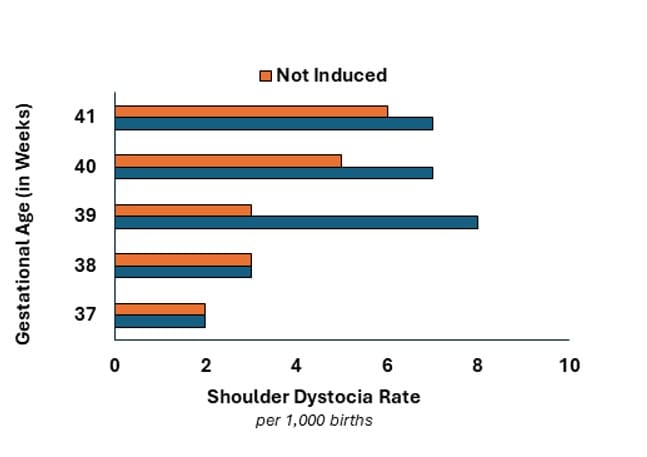
HQI’s analysis, however, shows a different trend: Late induction (post-39 weeks) is consistently associated with higher rates of shoulder dystocia (see Figures 1 and 2).
While a helpful tool if applied early, inducing delivery doesn’t erase risk entirely. The current practice of inducing before 39 weeks reflects a delicate balance; the longer a fetus that is large for gestational age remains in utero, the greater the risk of obstructed labor — but this must be weighed against the fact that induction itself carries its own hazards.
Among cases of shoulder dystocia from 2018–23, the rate of adverse outcomes increased half a percentage point if labor was induced — from 4.8% in cases without induction to 5.3% in cases where the delivery of the baby was induced (see Figure 3).

For clinicians, the heart of the issue is more than just intervention versus management — it is when to intervene. In patient safety, identifying risk is inseparable from understanding it. As hospitals work to improve care at their facilities, these data underscore that patient choice and clinical judgment must go hand in hand, since both action and inaction carry trade-offs and risks that require careful consideration.
